
By Yelena Baras, CNM
If you’ve had a visit with me in the clinic during or outside of pregnancy, you’ve inevitably heard me rant about how important it is to devote the proper amount of time and energy to your pelvic floor. You’ve heard me debunk the dominant social norms of the “tight” vagina being the more pleasurable vagina or that peeing yourself is sometimes “normal.” Many of our clients have been told by friends, trusted family members or previous providers that if they just did 1,000 kegel exercises a day, all of their problems during sex would be solved. Others believe that they will never be able to pick up their toddler again without the feeling of weakness in their abdomen. And of course, there’s that playground conversation amongst mom friends, all of whom pee themselves just a little on the trampoline, which seems warranted after a few kids.
I’m a big believer in asking for help, and since the pelvic floor is not my expertise, I interviewed local Pelvic Floor Physical Therapy Specialist, Genevieve Richter, PT, MPT, DPT, of Method Physical Therapy to help us understand the anatomy of the pelvic floor, the benefits of therapy, and the long term consequences of neglecting your lower half. Here are some answers to some common, important questions.
What is the pelvic floor?

The pelvic floor is “a dome-shaped muscular sheet separating the pelvic cavity above from the perineal region below.”1 The pelvic floor muscles function together with the surrounding bones, ligaments and soft tissues to contain the bladder, urethra, intestines, rectum, uterus, cervix, and vagina. The pelvic floor is often described as a “sling” or a “hammock,” whose primary functions are to support the abdominal and pelvic organs, to maintain control of the bladder and the rectum, and to allow for sexual activity and childbirth. Toward the front of the body, the pelvic floor muscles are connected to the abdominal muscles (the transverse abdominis and rectus abdominis), and towards the back of the body, they are connected to the lower back muscles.2 The pelvic floor is made up of three layers and each of these layers contain five or more different muscles, making this sling a complex and interdependent system. No wonder there are so many different pelvic floor dysfunctions and resulting discomforts that are treatable through pelvic floor physical therapy!
Who needs pelvic floor physical therapy?
There are many day-to-day reasons to be evaluated by a pelvic floor physical therapist. The most commonly-known reason is pain during sex, also called dyspareunia. According to a 2009 study, 10-20% of women in the United States report pain prior to, during, or after sex, including positional, vaginal, cervical, or penetrative pain.3 Dyspareunia can result from experiences of sexual assault or abuse, tissue damage from labor and birth, hormonal changes, rigorous physical activity, or conditioning from incorrect pelvic floor exercises or use of pelvic tools. The good news is that pain during sex is treatable and does not need to be tolerated! Some of these discomforts can be treated easily with lifestyle choices such as utilizing the correct lubricant and position changes during sex. However, many people with vaginas who experience pain during sex could benefit from a more extensive exam of the muscles, ligaments, soft tissues and bones that make up the “pelvic bowl” and are involved in sex. The pelvic floor physical therapist would identify the potential cause of pain, whether it is tightness versus weakness, activation of specific nerves, tissue damage or inflammation, muscular compensation, etc., and then offer solutions in the form of therapeutic touch, practice exercises, and/or use of tools.
Other reasons to see a pelvic floor physical therapist include urinary or fecal incontinence, bladder irritability (for example, interstitial cystitis), uncontrolled flatus (gas in or from the stomach or intestines), Irritable Bowel Syndrome, gastrointestinal discomfort, period cramps, and recent abdominal surgery (for example, gallbladder removal). Urinary incontinence is the leaking of urine when suddenly straining your muscles, called stress incontinence, or having the overwhelming urge to urinate prior to making it to the toilet, called urge incontinence. According to a 2018 study, 35% of women who have never been pregnant experience some kind of leaking of urine… and many of them think it’s normal!4 The truth is that no amount of leaking of urine is normal, whether it happens during your regular exercise, that time you jumped rope, or whenever you laugh or sneeze. Depending on the study, 10-30% of women who have never had incontinence before experience incontinence after their first pregnancy.5 As many as 15-25% of women experience urinary incontinence after multiple pregnancies.6 It is recommended to treat incontinence prior to becoming pregnant and in preparation for pregnancy, but it’s also completely safe to treat during and after pregnancy. I’ve heard many people say some version of the statement, “Well, what’s the point of treating this now, since it will just get worse during pregnancy? I might as well wait until I give birth and then I will deal with it.” But in reality, the longer you wait to be evaluated for incontinence, the longer your muscles are being conditioned incorrectly and the longer it may take to re-teach them. The earlier you can be evaluated and treated for the leakage of urine, the less risk there is for long-term consequences such as infection, prolapse, and pain.
Additional indications for pelvic floor therapy related to pregnancy are pubic bone and tailbone pain, sciatica, extensive tearing during birth (such as development of scar tissue after stitches, 3rd or 4th degree tear), cesarean section, prolapse, and persistent separation of the abdominal muscles called diastasis recti.
What does pelvic floor physical therapy look like?
When you come into the office of a pelvic floor physical therapist, they will get a comprehensive history of your reasons for seeking out therapy, eating and drinking habits, physical activities, when and if you experience pain during tampon use and/or sex, and how many times you go to the bathroom in a day.
The therapist will begin the physical evaluation by testing or measuring how you move your body including hips, legs, and abdomen. Next, with your consent, the therapist would prepare for an internal physical exam by setting up a table with a sheet and having you undress from the waist down. The internal examination is very similar to, but also more detailed than the one you have annually with your midwife. They would begin the internal exam by using a glove and lubricant to insert one finger into the vagina to assess the general muscle symmetry, strength, length, tone, contraction and relaxation ability. The therapist might instruct you to squeeze your vaginal muscles as if you were going to stop the flow of urine, also known as a “kegel.” The therapist may repeat these exercises multiple times with their finger in different positions inside of the vagina or you in different positions (lying down, sitting or standing) to test how long and how many times you are able to hold the muscle contraction. Then they will ask you to bear down, pushing out like you were going to pass gas or have a bowel movement. This is to check for your ability to lengthen or relax the musculature. They may also feel the muscles for knots or areas of pain in order to identify the muscle, ligaments, tissues that may be causing your symptoms, discomfort, or tenderness. Lastly they would assess the position of the bones and organs inside of the pelvis such as the tailbone, pubic bone, bladder, cervix, vagina, and rectum. Sometimes therapists use tools during their assessments, such as a biofeedback machine which measures the amount of muscle stress or tension you are exerting while doing an exercise. Depending on the therapist portions of the assessment may happen in a different order.7

What will the pelvic floor physical therapist recommend after my evaluation?
Each person’s needs are different when it comes to the treatment of pelvic floor dysfunction. The goal is to help you learn how to use your pelvic floor muscles most efficiently and safely. Depending on your evaluation and goals, the pelvic floor physical therapist may recommend exercises to help you relax or strengthen your pelvic floor muscles. These may include abdominal exercises (e.g. planks, twists, legs lifts, and pelvic lifts), breathing exercises, fast and slow kegel exercises, and reverse kegel exercises. In addition, the therapist may offer the use of medical tools in your treatment plan such as dilators, biofeedback machines, or pelvic trainers. It is important not to use these tools unless recommended by your therapist, since they can cause further damage to your pelvic floor if not used correctly!
The therapist will likely recommend that you don’t engage in high impact exercise such as running or weight lifting until at least 3 months after your birth or longer, until your pelvic floor is adequately healed to prevent long-term injury.
Does everyone get that abdominal muscle separation during pregnancy?
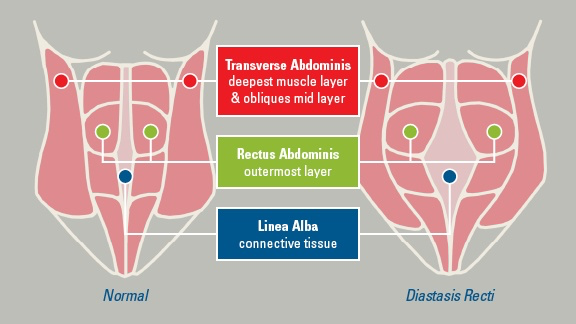
All women will experience some level of separation in their abdominal muscles during pregnancy that may persist after birth. The growing uterus is helped by the hormones of pregnancy (estrogen and relaxin) in causing a thinning and a separation of the outermost layer (rectus abdominis) and the deeper layer (transverse abdominis). This results in a stretching out of the linea alba, the connective tissue between the muscles.
It is unclear what amount of separation is normal versus abnormal. Studies show that the average separation of the rectus abdominis in non-pregnant people is less than 1.5 cm.8 It is common for women to have a diastasis recti of 1-2 cm (1-2 finger breadths) that persists for 3-6 months after birth and resolves on its own. However, if the separation remains 2 cm or more with very distinct borders and/or with a “doming” or “coning” of the muscle at 3 months after birth, then it’s time to make an appointment with a pelvic floor physical therapist. It’s really important to have your persistent or extensive diastasis recti evaluated before starting to exercise to ensure that the exercises you’re doing do not make the separation worse or prolonged.9
I heard that stronger pelvic floor muscles are healthier and doing kegel exercises will prevent me from peeing myself in the future. Is this true?
Not always! Some women experience pelvic pain prior to, during, or after sex, because their pelvic floor muscles are hypertonic — meaning too tense or unable to relax. Sometimes this is caused by high impact exercise, a history of sexual trauma, or musculoskeletal injuries. In this case, relaxation exercises may actually be the solution. This is why it is important to be evaluated by a pelvic floor physical therapist before assuming that kegel exercises are right for your body type.
I am not planning a pregnancy now, or maybe ever. Do I still need to have pelvic floor physical therapy?
Absolutely! As mentioned above, there are many reasons why a person who is not currently pregnant or not planning a pregnancy may want to seek out pelvic floor physical therapy. Everyone deserves to urinate only when they want to, have pain-free sex, and avoid exercise-induced injuries. If you are planning a pregnancy in the future, it is ideal if you can train for pregnancy by getting your pelvic floor in shape with the help of a pelvic floor physical therapist a few months prior to conception.
I am already pregnant, should I just wait until after I give birth to start physical therapy?
It is highly recommended that you start pelvic floor physical therapy as soon as you notice a problem. And yes, this means during pregnancy! For women who have hypertonic pelvic floor muscles, receiving treatment during pregnancy will help them relax the pelvic floor during pushing, thus decreasing risk for more extensive tearing and longer pushing. Women who have incontinence during pregnancy and receive pelvic floor physical therapy are less likely to experience it after the pregnancy.
You can sign up for Genevieve’s next online Pelvic Floor class through Dar a Luz HERE. Let us know if you have any questions. Here’s to your healthy pelvic floor!
Yelena

Yelena Baras, CNM, was born in Samara, Russia and immigrated to Philadelphia, PA, when she was 4 years old. She always knew that she wanted to work with women, to be an advocate for reproductive rights and contraceptive choices. She is excited to be part of the family at Dar a Luz. She comes from a background of wellness nursing, and is interested in supporting our clients in making positive and informed healthcare decisions. She has studied several types of yoga, including Vinyasa and Acroyoga, and practices meditation both in individual and group settings. She enjoys spending her weekends on hikes and camping.

Genevieve Richter, PT, MPT, DPT, is an Air Force brat that has lived in Albuquerque for the past 20 years. She graduated from UNM in 2010, and has specialized in pelvic health for the past 10 years. She has a huge passion for treating under-represented patient populations that suffer from pelvic dysfunction, as well as a strong focus on pregnant and postpartum rehabilitation. Genevieve is just as passionate about raising her two young children and working in the yard with her husband. Her website can be found HERE.
- Bharucha, A.E. (2006). Pelvic floor: anatomy and function. Neurogastroenterology & Motility. 18(7):507-19.
- Yates, A. (2019). Female pelvic floor 1: anatomy and pathophysiology. Nursing Times [online]; 115: 5, 18-21.
- Sorensen, J., Bautista, K. E., Lamvu, G., & Feranec, J. (2018). Evaluation and Treatment of Female Sexual Pain: A Clinical Review. Cureus, 10(3), e2379. https://doi.org/10.7759/cureus.2379
- Daly, D., Clarke, M., & Begley, C. (2018). Urinary incontinence in nulliparous women before and during pregnancy: prevalence, incidence, type, and risk factors. International urogynecology journal, 29(3), 353–362. https://doi.org/10.1007/s00192-018-3554-1
- Wesnes, S. L., Hunskaar, S., Bo, K., & Rortveit, G. (2009). The effect of urinary incontinence status during pregnancy and delivery mode on incontinence postpartum. A cohort study. BJOG : an international journal of obstetrics and gynaecology, 116(5), 700–707. https://doi.org/10.1111/j.1471-0528.2008.02107.x
- Handa, V.L. (2015). Urinary incontinence and pelvic organ prolapse associated with pregnancy and childbirth. UpToDate. http://enjoypregnancyclub.com/wp-content/uploads/2017/06/Urinary%20incontinence%20and%20pelvic%20organ%20prolapse%20associated%20with%20pregnancy%20and%20childbirth.pdf
- Lough, K. (2015). Physiotherapy first for pelvic floor dysfunction. https://www.urologynews.uk.com/features/features/post/physiotherapy-first-for-pelvic-floor-dysfunction
- Physiopedia. Diastasis Recti Abdominis. (n.d.). https://www.physio-pedia.com/Diastasis_Recti_Abdominis
- Brancato, D. (2015). Diastasis Recti: Not Just For New Borns and Pregnant Women. https://www.nfpt.com/blog/diastasis-recti-not-just-for-new-borns-and-pregnant-women
Latest Articles

Special Newsletter: Ketamine Infusion Therapy

Special Newsletter: Teen Services!
